


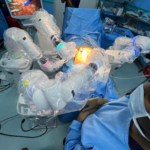






Patients with clinically localised prostate cancer are treated with a robotic laparoscopic prostatectomy. The vast majority of patients who qualify for an open radical prostatectomy also make great candidates for the robotic procedure. The robotic technique is the surgical therapy strategy of choice at many centres, including the University of Florida, for clinically localised prostate cancer.
Even though it happens very seldom, conversion to open surgery can be necessary if the robotic method encounters problems with dissection or significant bleeding. Our doctors are skilled in both openRobotic prostatectomy may not be the ideal option for patients with a history of major abdominal surgery, radiation, underlying heart or lung illness, morbid obesity, or bleeding tendencies. Robotic prostatectomy is not an option for patients with known metastatic or recurring prostate cancer. Although patients with extremely big prostate glands (e.g., > 100 grammes) are still eligible for robotic prostatectomy, the procedure typically takes longer than it does for people with lesser prostate gland sizes. and laparoscopic procedures, as well as robotic surgery, so they are prepared to complete the procedure either way, if necessary.
Even though it happens very seldom, conversion to open surgery can be necessary if the robotic method encounters problems with dissection or significant bleeding. Our doctors are skilled in both open and laparoscopic procedures, as well as robotic surgery, so they are prepared to complete the procedure either way, if necessary.
Following a prostatectomy, the extent and timing of the recovery of sexual function and continence is a complicated process that depends on numerous factors throughout time. Age, preoperative sexual and urogenital function, and the existence of medical diseases including diabetes and hypertension are some of the patient characteristics that affect the success of returning these quality-of-life difficulties. Additionally, surgical elements like the degree and scope of nerve preservation can affect results.
At 6 and 12 months, respectively, 73% and 88% of young patients (60 years old), who were preoperatively potent and had no urinary problems, were continent (defined as 0-1 security pad), and 87% and 93% were potent (defined as having the ability to engage in intercourse with or without the use of phosphodiesterase inhibitor medications). The degree of the malignancy, the patient's age, and any coexisting illnesses can all have a substantial impact on these outcomes. Please refer to the graphs of results for potency and continence above.